How can rebreather diving be made safer? That was the question at the core of the numerous presentations and discussions at Rebreather Forum 3 (RF3) held in Orlando, Florida, this May.

Contributed by
The last forum, Rebreather Forum 2.0, which I organized with rebreather builder Tracy Robinette, was held 16 years earlier in 1996, at a time when rebreathers were just being introduced to the sport diving market.
In his opening remarks, PADI CEO, Drew Richardson, proposed that the number one goal of RF3 was contributing to rebreather diving safety and reducing incidents.
Some controversy
The issue is of critical importance today when manufacturers like Poseidon Diving Systems Ltd. and Hollis Inc., in conjunction with PADI and other training agencies, are now actively promoting rebreathers for use by recreational divers, which is a source of some controversy. Until recently, rebreather use was limited primarily to tech divers because of their complexity, operational requirements and cost. The concern is that rebreathers may be too complex and time consuming for a typical open water diver who is still mastering their basic diving skills.
A matter of protocol
However, PADI has developed a simplified diving protocol using rebreathers designed specifically for recreational use, which it believes will prove efficacious.
Though no one knows the actual risks, there have been more than 200 reported rebreather fatalities worldwide since 1998, which have averaged approximately ten fatalities per year prior to 2005 and about 20 per year since. To put these numbers in perspective, on average there are about 100-120 scuba diving fatalities annually in the United States, Canada, United Kingdom and Europe combined, which represents the majority of the worldwide market.
Given that there are millions of open-circuit divers compared to, at most, tens of thousands of rebreather divers, the fatality rate for rebreather diving is evidently much higher than its open-circuit counterpart, as industry-insiders are all too well aware.
Unacceptable record
During one of the opening sessions, Dr Andrew Fock, head of hyperbaric medicine at The Albert Hospital in Melbourne, Australia, asked for a show of hands from the audience: “How many people in this room believe that the current rebreather safety record is acceptable?”
No one raised a hand.
Conceived centuries ago
First conceived in the 17th century by Giovanni Borelli, closed-circuit rebreathers (CCR) remained an elusive invention until the advent of galvanic oxygen sensors in the early 1960s made their construction possible. Like simple, non-electronic oxygen rebreathers before them, the technology was primarily limited to military divers until the late 1980s when pioneers like Dr Bill Stone, Olivier Isler, Stuart Clough and Rob Palmer began experimenting with rebreathers for cave exploration, just as technical diving was emerging.
Though the early tech community immediately seized upon their potential for extending bottom times and optimizing decompression, it took until the late 1990s for the first production units like the Cis-Lunar Mk-IV, Ambient Pressure Diving’s Inspiration and the KISS Classic to become available.
Fastest growing segment
Today, rebreather diving represents one of the fastest-growing areas of sport diving. Poseidon reported at the Forum that they sold more of their recreational Mk-VI rebreathers in the last four and half months than in the prior two and half years, and PADI is certifying new recreational rebreather instructors to meet the demand. In certain countries, such as the United Kingdom, which is regarded as rebreather “ground zero”, it’s considered “normal” that everyone on a dive boat is diving a rebreather.
Industry insiders estimate there are as many as 10,000 to 15,000 active rebreather divers worldwide, and there are more than a dozen rebreather manufacturers.
At one of the forum sessions, the three oldest technical training agencies, ANDI, IANTD and TDI, which have been responsible for the majority rebreather training to date, estimated that collectively they issued 30,000 basic, intermediate and advanced rebreather certifications from 1990-2011, and are currently trending at about 2,500-3,000 certifications a year. (Data from the British Sub-Aqua Club, PSA International, and Rebreather Association of International Divers was not included).
These numbers are likely to grow significantly as PADI recreational rebreather courses proliferate.
Though the number of users is still small, rebreather technology has greatly expanded tech divers’ underwater envelope, and has also been a boon to photographers/videographers as well as the early adopters among scientific and recreational divers as evidenced by the community’s sessions chaired by explorer and instructor trainer Martin Robson.

Pushing the envelope (again)
Dives that would be logistically difficult or even impossible on open-circuit are routinely done with rebreathers, and some explorers like Robson, Richard Harris and others are now pushing limits of human physiology. During a Friday afternoon session, Harris detailed his team’s exploration dives to 207m (680-feet) at the Pearse River Resurgence (caves) in the South Island of New Zealand, where divers are hitting up against the limits of “respiratory sufficiency” (and arguably surface-based diving).
However, as David Conlin, Chief of Submerged Resources Center for the National Park Service, explained to the assembly, “The real value of rebreathers is not deep diving at all, but staying longer at 21-30m (70-100 feet). You can work at those depths nearly all day long when the conditions are good.” Conlin reported that rebreathers have increased Park Service divers productivity by nearly 40 percent. “We gain nearly one day for every three days we’re in the field.”
Killing them softly
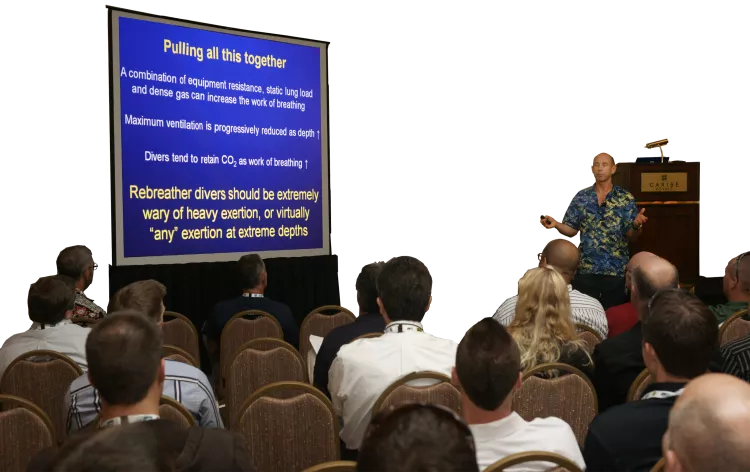
Fock, who himself is a very accomplished rebreather diver, took the stage on Saturday morning with an important and sobering presentation on the risks of rebreather diving, titled, Killing Them Softly. One of the problems in the industry is the lack of an accident reporting system that records and details the cause of diver fatalities and near misses, in order to inform and improve diver safety. In many cases, information about specific fatalities is sequestered for fear of litigation.
As a result, existing accident data is incomplete, and in many cases, inaccurate.
Fock analyzed available data from multiple sources from 1998-2010 to answer some basic safety questions like:
- How dangerous is rebreather diving?
- What causes fatalities?
- Are manual units (that depend on the diver to manually add oxygen)—like the KISS Classic, which represents about 15 percent of the installed base of rebreathers—safer to dive than their electronic counterparts?
- Are there any specific brands of rebreathers more dangerous than others?
- And finally, is the risk reduced when diving within the recreational envelope (i.e. no-stop diving to 40m or 130ft)?
With the caveat that they are “best guess numbers”, Fock concluded that rebreather diving is probably 5-10 times as risky as open circuit scuba diving, accounting for about 4-5 deaths per 100,000 dives, compared to approximately 0.4 to 0.5 deaths per 100,000 dives for open-circuit scuba.
This makes rebreather diving riskier than sky diving at 0.99 per 100,000 jumps, but far less risky than base-jumping at 43 deaths per 100,000. He found that there was no difference in fatality rates among manual or electronic units or specific brands of rebreathers; accidents were roughly proportional to market share. Fock also pointed out that while the data suggests that deeper dives carry greater risks, a large number of rebreather fatalities occur in shallow depths within the recreational envelope.
“Pilot error”
As far as the causes or “triggers” that precipitated accidents, Fock concluded that the source of most problems was the human-machine interface, or so-called “pilot error”, involving assembly and pre-dive preparation, maintenance, training and high risk behaviors like ignoring checklists, carrying insufficient bailout and diving beyond one’s limits. “The question,” posed Fock, “is whether the risk can best be mitigated by training [reinforced by dive culture] or engineering out potential problems or both.”

Creating a safety culture
Though veteran explorers and educators Jill Heinerth and Terrence Tysell chaired an open-discussion session on training, enabling Forum participants to present views on a host of training related topics, the majority of the discussion on improving safety centered around diving culture—what happens after training.
Currently, one of the biggest safety issues surrounding rebreathers is the fact that divers become complacent and don’t rigorously adhere to a pre-dive checklist in assembling and preparing their unit for diving as they (presumably) learned in class, and also neglect required post-dive maintenance. (Some experienced rebreather divers don’t follow checklists either.) Even worse, some divers choose to dive knowing that there are problems with their unit such as a faulty sensor or small leaks.
Methodically working through your rebreather’s checklist, which typically includes a five-minute pre-breathe (and only diving it if everything checks out), is the best way to insure that the unit is functioning properly and avoid any problems that could jeopardize safety during the dive. The use of checklists is standard in aviation and is increasingly becoming so in medicine, because it reduces accidents. Presenters saw the problem as an issue of creating a safety culture to support rebreather diving.
Expedition leader and educator Richie Kohler made an impassioned, no-nonsense case for the use and efficacy of checklists in his presentation, Failure Is NOT an option: The importance of checklists. During the presentation, Kohler put up a picture of eight close friends and mentors including his rebreather instructor, who lost their lives as a result of pilot error. “They were not fools,” explained Kohler, “but each of them made foolish mistakes and died as a result.” Checklists are designed to prevent such mistakes from occurring.
In another session, Heinerth presented her “Five Golden Rules” for rebreather diving which included:
- be properly trained and current for the dive you are about to conduct;
- follow your checklist;
- pre-breathe your unit;
- make the decision to dive (responsibly); and
- be prepared to abort the dive safely (with sufficient bailout gas!). Heinerth told a story of being on a dive boat with five rebreather veterans.
During her pre-breathe, she detected a small problem with her rebreather and told the assembly she would be sitting out the dive, only to be pressured by the others divers to make the dive anyway. “It’s only a minor problem,” some opined, “You can still fly the unit manually.” To her credit, Heinerth didn’t back down.
How do we, as a community, encourage divers to do checklists and support their adoption within the culture?
“Industry leaders need to become role models,” offered Heinerth. “We need to make it cool to do checklists.”
Heinerth along with industry pioneers Dr Richard Pyle, Database Coordinator for Natural Sciences at Bishop Museum, Kevin Gurr, CEO of VR Technology, and others are now spearheading an effort to create a set of best practices for rebreather diving dubbed, Blueprint For Survival 3.0.
This refers to the original set of ten safety principles for cave diving developed by legendary cave explorer Sheck Exley in his monograph, Basic cave diving: A blueprint for survival. The early tech community created a similar set consensus-standards for open -circuit mix diving, Blueprint for Survival 2.0, which was published in the now-defunct aquaCORPS Journal. Watch this space.

Engineering the CCR blues away
In addition to training and creating a culture that reinforces safe diving practices, experts agree that a number of safety issues might be resolved through better engineering. Indeed, this is the basis behind PADI’s so-called “Type R” rebreathers that are suitable for recreational divers. For example, a Type R rebreather will turn itself on if the user forgets and jumps in the water, and it won’t operate without the scrubber canister correctly in place or if the cylinders are turned off.
What became clear at the Forum, however, is that better engineering solutions are needed for one of the most fundamental aspects of rebreathers: knowing precisely the composition of the breathing gas in the loop at any point in the dive. Unlike open-circuit, of course, where the fraction of gas is constant and known with certainty, the gas mix in a diver’s breathing loop dynamically changes with every breath and gas addition.
Ten to 15 years from now
Ten years from now, or 15, we will likely look back at our current technology and regard it as primitive, or what explorer and engineer Dr Bill Stone, CEO of Stone Aerospace, refers to as “test pilot era” technology. “You actually dived those units without knowing exactly what you were breathing? OMG!” It’ll be like us looking back at early cave divers using J-values (reserve) and empty Clorox bottles for buoyancy, and going, “Really?”
Bruce Partridge, CEO of Shearwater Electronics, summed up the current state of the art in his presentation on information systems this way, “Divers must interpret the readouts from three roaming O2 sensors, which are known to be unreliable. They dive with no CO2 gauge, and they don’t have good data on the risks or what is most likely to go wrong.”
The trouble with O2 sensors
Most experts agree that current O2 sensing systems are the weakest links on a rebreather and also the most critical. If the PO2 in the loop is too low, the diver will suffer hypoxia and go unconscious and drown; too high and the diver risks hyperoxia, convulsions and drowning.
Limits
But what most divers might not appreciate are the limitations of current O2 sensing systems on the market, which was made clear in a pair of presentations by biomedical instrumentation engineer Dr Arne Sieber, CEO of Seabear Diving Technology who built his own rebreather, and Nigel Jones, principal at RMB Consulting who works with Stone Aerospace.
Sensors were not designed with diving in mind
Sieber began by explaining that the galvanic O2 sensors made for the biomedical industry were never designed to be used in diving and are, in fact, being used outside the manufacturer’s specs. To wit: sensors are meant to be calibrated under the same conditions that they will be used for in measurement, in the same measurement range and temperature. That’s not how it’s done in diving.
“Divers do all the wrong things,” explained Sieber. “We calibrate the sensors at 0.2 bar (air) and 1.0 bar (O2) at ambient pressure and temperature, and then use the sensors at up to 1.6 bar at much hotter temperatures,” Sieber said that this leads to increased sensor errors as well as a decreased lifespan.
Sensors can fail high or low as a result of the gradual consumption of their reactive material and ageing and also fall out of calibration. In addition, they commonly fail from condensation on the sensor. Worse is that “transient failures” from a loose electrical connection, or more commonly condensation, causes the sensor to generate erroneous data and then go back to working correctly when the condition abates. Jones believes that these “transient failures” are insidious and likely the cause or trigger of many unexplained rebreather diver fatalities.
Voting logic
Because of the known unreliability of these sensors, early designers like Walter Stark in the late 60’s who invented the “Electrolung” built the first closed-circuit rebreathers with three O2 sensors and a voting logic algorithm—the computer averages the readings from the two sensors whose readings are closest and uses that average for its O2 calculations.
Their idea was that the redundancy of three voting sensors would greatly reduce the risk of sensor failure, and the concept stuck. Today, virtually all rebreathers, except the Poseidon, use this 50-year-old sensing technology. The problem, explained Jones, is that it is simply not as reliable as once thought.
Reducing the benefits
First, Jones showed using probability theory that the voting logic algorithm itself actually reduces the benefits of redundancy. For example, instead of having a system that is “hundreds” of times more reliable (e.g. with pure triple redundancy), a voting logic system can reduce the improvement to single digits.
Questionable assumption
Second, voting logic is based on the assumption that sensors fail independently i.e. the failure of one sensor does not change the likelihood that others will fail, too. Unfortunately, that is not the case with the O2 sensors in a rebreather. The sensors are dependent because they share a common history; they may have come from the same manufacturers' lot, they experience similar use, they share a common environment, suffer common abuse and use shared measurement and calibration gas. The lack of independence greatly decreases reliability. “Having three sensors is barely better than one in some circumstances,” emphasized Jones.
Erosion of risk reduction
Third, risk reduction is eroded even further, by the fact that there are more than two outcomes to the system i.e. heads: a correct reading, or tails: an incorrect reading. The third outcome is the case when the diver doesn’t know if the reading is correct or incorrect, which Jones equated to having the coin land on its edge.
Case story
He offered a real-world example reported by Rich Pyle where during a dive, his PO2 sensors read .4, 1.0 and 1.3 and asked the audience to make the call, “What is the correct PO2?” (The computer’s voting logic would average the 1.0 and 1.3 reading and call it 1.15).
Unfortunately, the majority of the audience got it wrong! The correct answer was 0.4; the system had experienced a double sensor failure. Fortunately, Pyle got it right. If he had ascended at that point in the dive thinking his PO2 was 1.15, he would have risked hypoxia and possible drowning.
Calculations under duress
An animated discussion ensued prompted by Leon Scamahorn, CEO of Inner Space Systems and manfacturer of the Megalodon and Pathfinder rebreathers, who pointed out that “Meg” users could go the “millivolt screen” on their handset, which shows actually sensor voltage (a linear function of PO2) and with some simple math determine that the low sensor was correct. This assumes of course that the diver was alerted to the problem in time. [Scamahorn’s arguments, however, did not address the limitations of voting logic systems].
I’m sure Pyle, who has thousands of hours on his rebreather, wouldn’t have a problem with Scamahorn’s procedure (Pyle was tipped off to the faulty sensors by the lack of voltage fluctuations). But I couldn’t help wondering if I’d have the calm presence of mind do “millivolt math” at 100 meters with the stress of a possible alarm and knowing one or more of my sensors were crapping out. Definitely a test pilot-esque notion! Couldn’t a computer do this better than me?
Active validation
Both Sieber and Jones urged the industry to develop and adopt “active validation” type systems, such as used in the Poseidon MK-VI, which calibrates and tests the validity of the oxygen sensors (the MK-VI uses two sensors) throughout the dive using onboard diluent and oxygen. Sieber added that solid-state sensors, which are currently in prototype form, also hold promise for the future.
However, several rebreather builders I spoke to disagreed with Sieber and Jones’ assessment and said that they overstated the O2 sensing problem given improvements in sensor manufacturing, testing and voting logic software. As one manufacturer said, “There’s more than one way to skin the cat.”
Nevertheless, in its consensus recommendations, the Forum strongly endorsed industry initiatives to improve oxygen measurement technologies and advocated consideration for new approaches like “active validation” and alternatives to galvanic fuel cells.
ppCO2: The dark matter of rebreather diving
Divers face similar sensing problems with respect to pCO2, which has been dubbed the “dark matter of rebreather diving”. High ppCO2’s (0.03 bar and above) can cause hyperventilation, confusion, mental impairment, unconsciousness and death, may lower CNS O2 toxicity thresholds and is believed to be a factor in unexplained rebreather fatalities, hence the moniker “dark matter”. Worse, the diver may not be aware of the problem before a full onset of symptoms occurs.
Searching for 25 years
According to Dr John Clarke, Scientific Director of the U.S. Navy Experimental Diving Unit (NEDU), the Navy has been searching for solutions to problem of CO2 sensing for more than 25 years. The need for CO2 sensing was also identified in the findings of Rebreather Forum 2.0.
Divers have two information needs: first, to monitor the duration of the scrubber canister, which varies with workload, depth, and temperature; second, to detect a CO
breakthrough as a result of a spent canister, mechanical failure or channelling.
Ignorant divers
Kevin Gurr, who is regarded as one of the gurus on CO2 sensing, began his session by sharing data from a recent Internet survey of 323 rebreather divers representing 25 different models of rebreathers. The results were surprising. Twenty-three percent of the divers did not know the maximum operating depth of their unit, and another 19 percent did not know the manufacturer’s stated scrubber duration. Forty-two percent of divers said that they experienced symptoms of hypercapnia for a total of some 297 incidents (some divers had more than one incident), however, 64 percent said that they didn’t bailout; 19 percent said they bailed out sometimes. The results suggest better training and a cultural shift are needed!
Gurr next recounted the current methods used to monitor scrubber duration which are: 1) a duration timer based on manufacturer’s test data (usually conducted at two depths at 4ºC at a specified CO2 production rate); 2) a timer system based on the diver’s oxygen consumption (divers produce about 0.8 liters of CO2 for every liter of O2 consumed) which takes account of workload but not depth or temperature; and 3) thermal sensing, also referred to as the “Temp Stik”, which measures how the scrubber’s thermal reaction front moves through the canister. Gurr explained that the Stik, which is used in the Ambient Pressure, VR technology and rEVO rebreathers, is a reasonable predictor of duration, but is slow to react to fast changing variables like work rate. However, none of these methods are able to detect CO2 breakthrough!
Following Gurr, Dr Dan Warkander, from the Navy Experimental Diving Unit (NEDU) who holds a patent on thermal sensing, compared to the days of early scuba when divers didn’t have a pressure gauge but instead dived with a J-valve. “Wouldn’t it be nice to have a gauge for your scrubber to tell you how much time you had left?” he offered.
Warkander went on to explain how factors such as workload, depth and temperature effect scrubber duration and how difficult it is to predict. For example, hard work can reduce duration by 50 percent, while light work can double duration. He said that scrubber duration can vary by a factor of 5-20 through combined effects of workload, temperature and depth. What’s worse, when a scrubber is spent, the threshold between no CO2 and too much, can happen in a matter of minutes.
As far as detecting scrubber breakthrough or a seal failure, VR Technology Sentinel is currently the only production unit with a gaseous infrared CO2 sensor (The Sentinel uses all four methods mentioned above in its CO2 monitoring package). Gurr said that we are 80 percent there in fully characterizing a CO2 absorption system properly.
Holy grail
The last piece is a mouthpiece sensor that can measure end-tidal CO2, which is regarded as the “Holy Grail” of CO2 monitoring. Gurr estimated that this is still at least three years away.
The Forum acknowledged the poor of understanding of operational limits with regards to depth and scrubber duration among trained rebreather divers and recommended that training agencies do more to emphasize these issues, and manufacturers make data more readily available.
Dive-by-Wire?
The diving press and interested Forum participants were treated to a preview of Poseidon and Stone’s latest lovechild, the Poseidon TECH rebreather, which is scheduled to ship this November and features the latest in diving automation. “Our goal,” explained Poseidon CEO Peter Swartling at the press briefing, “is to increase the level of automation by using smart systems that monitor every breath, make adjustments accordingly and interact with the user only when they need to know what’s going on.”
In addition to the many automated features in Poseidon’s Mk-VI recreational rebreather such as a wet switch, an auto-checklist that verifies that cylinders have the correct gases and their values are open, and auto-oxygen sensor calibration and validation, the new TECH offers a “Dive-by-Wire” handset that is truly breaking new ground.
The device, which is smaller than an iPhone, provides system information to the user and enables them to control the rebreather to the extent of doing a loop flush or adding oxygen at the touch of a virtual button. The computer of course would warn and or prevent the diver from taking an action, like adding O2 if it was ill advised.
This level of automation gave heebeegeebees to many of the tech divers I spoke with at the bar following Poseidon’s press conference, but I couldn’t help wondering if this is indeed the future of dive automation. Granted, 15 percent or so of rebreather divers prefer a strictly manual unit (sans solenoid) and other groups such as the DIR community don’t even trust dive computers, well not the kind that you strap to your arm anyway. Ironically, I’m sure that most of these people have no trouble trusting their ABS brakes in their cars (versus feathering the brakes on their own). In fact, their vehicles depend on computer automation, as do the commercial aircraft that flew them to RF3.
Can we trust automation?
Stone, whose company builds autonomous vehicles for space exploration, addressed the issue head on in his talk, Hazard Analysis and Human Factors, posing the question, “Can we trust automation?” As an example, he recounted the development of the autonomous car that can navigate city streets sans driver and showed video of prototypes in action. Stone said that within five years, you’ll be able to buy a car that will drive you home if you had a bit too much to drink, and it will do it as safe or safer than a human driver.
Could rebreathers be far behind?
One of the major problems in rebreather (read car, train, plane, spacecraft, etc.) safety is humans’ ability, or rather inability, to manage and operate complex machines without incident. Stone’s solution, along with others such as Gurr’s soon-to-be-released Hollis Explorer, is to simplify the human-machine interface by reducing the ways that people interact with these systems, letting the computer do more of the work. “We have to move out of the test pilot era to a new paradigm,” he said.
Given that Stone’s vision of more than 25 years ago helped drive the creation of a consumer rebreather market (he could arguably be considered the godfather of modern rebreathers) his ideas should not lightly be dismissed.
At the closing session of the forum, just before Dr Simon Mitchell, who heads the department of anaesthesiology at the University of Auckland, New Zealand, brilliantly facilitated and crafted a series of community-consensus statements from the assembled Forum participants (no small task!), audience members were encouraged to speak out and share their views. Andrew Fock walked up to the mic and put the following question to the community, “Given that the fatality rates are five to ten times that of open-circuit scuba, should we morally offer this technology to the recreational diving community, before putting our house in order?”
There was silence as if no one wanted to tackle the question, then another participant took the stand and changed the topic. Eventually, Mark Caney, PADI’s Vice President of Rebreather Technologies, worked his way to the microohone and addressed his comments to Fock.
“Yes we should,” he said. “Within certain parameters.” ■
Writer and technologist Michael Menduno published and edited aquaCorps: The Journal for Technical Diving (1990-1996), which helped usher tech diving into the mainstream of sports diving, and coined the term “technical diving”. He also organized the first Tek, EuroTek and AsiaTek conferences, and Rebreather Forums 1.0 and 2.0. Menduno, who is based in Berkeley, California, USA, remains an avid diver.